Blog written by Hayley Lever
Why does the integration of physical activity and health matter to you and your work?
This question was the focus of a recent event, hosted by GreaterSport and Yorkshire Sport Foundation and supported by GM Moving partners, the Active Partnership Network and Sport England.
Why did we hold the event?
Effective delivery of Uniting the Movement requires collective leadership across sectors and across England. Connecting with Health and Wellbeing is one of the five big issues within this shared strategy. To play our part in the delivery of Uniting the Movement, we have been designing a more networked, integrated approach to our work- with a culture of collaboration and trust at its heart.
In short- we’re trying to work better together because it will help us to create better conditions to address inactivity and inequalities.
One of our collective priorities is a Health, Wellbeing and Inactivity Learning Approach: Connecting with ICS’ and Networks. The Active Partnership Convention workshop in March 2022 showed that there was a need and appetite for a learning and sharing network, so a small group of representatives from across organisations came together to shape up a programme of events and support for the year ahead, which we launched in June.
The first event in this new programme took place last week: a hybrid workshop in Manchester and on Zoom, with over 80 people in attendance from around the country and across sectors, entitled: Physical Activity and Health Integration: Learning in Action
Who took part?
Active Partnership and Sport England colleagues participated, as well as people from Sport England’s other system partners (such as Activity Alliance and the Richmond Group), health and care colleagues from the Office for Health Improvement and Disparities to Primary Care and Allied Health Professionals, and people from local government, community leisure providers, social enterprises and many more.
Event Purpose:
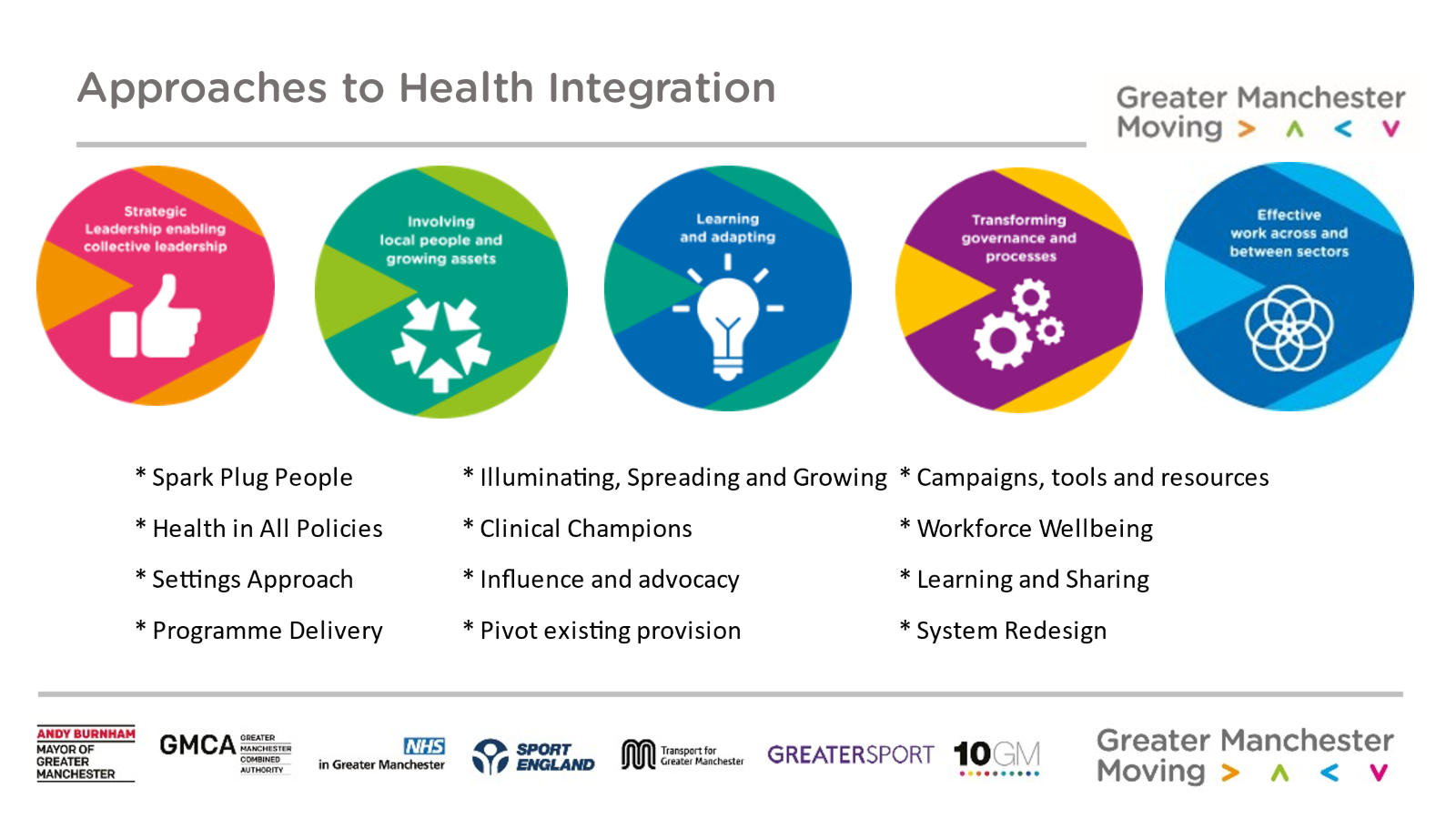
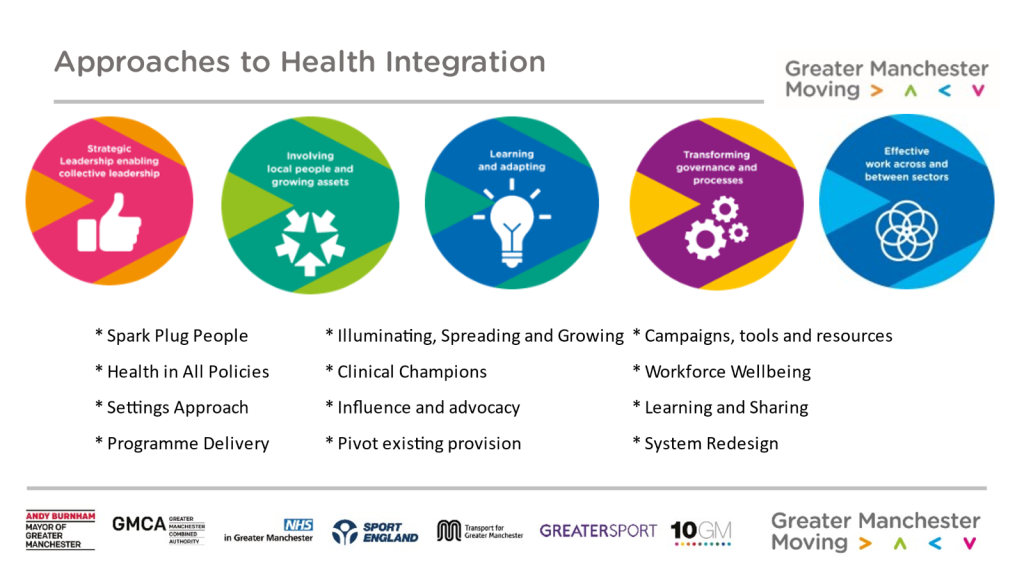
- To explore the approaches we’ve all taken so far to integrate health and physical activity.
- To hear from local leaders in the GM ICS, who will reflect on their personal leadership journeys as they have led this work from a health and physical activity perspective.
- To consider the evidence we have so far about what makes change happen.
- To reflect on the ways of working and approaches that we might take next, given our local circumstances and contexts.
- To develop personal, organisational and/or system intentions and actions to take back into our work.
This was done through a two-part event. A two-hour hybrid session in the morning, followed by a walk, wheel or scoot, then lunch and a deeper exploration via activities for those in the room.
This was the first hybrid event that the group have facilitated, so the process of developing the programme was learning in itself! From experience over the past few years, we know that all day Zoom is not a healthy or productive environment.
The afternoon was designed to enable relationship building for those attending in person, and to test out some activities to help with system mapping, storytelling, consider resource and support requirements and evaluate our role as influencers in our own systems. It would be interesting to host some of these activities as standalone events in the virtual world too.
If you were unable to join us or want to look back, recordings of the panel discussion and Q&A are now available to view, aswell as this blog for those who prefer to read.
Sharing Stories
To open the session, we heard about the strategic context and rationale for the session from Hayley Lever, Exec Lead for GM Moving and CEO of GreaterSport (Greater Manchester’s Active Partnership). She explained how GM Moving partners are taking stock after the first 5 years of devolution and health integration journey; capturing evidence, evaluation and learning as they shape the new ICS strategy which will launch in 2023.
Hayley said “it is important that we learn from our approaches to date, so that we can better understand what is helping to make change happen and how. Then we can become more effective and impactful as we continue to integrate physical activity, health and care in the next phase of the work”.
Hayley has written about this recently and the GM Moving evaluation partner, Substance Consortia, are now undertaking a deep dive evaluation alongside the development of the ICS strategy.
Conversations
Participants then spent ten minutes talking to someone on their table or breakout room, explaining what brought them to the session, why integrating physical activity and health matters to them and their work and sharing a bit of what they have been doing so far and why?

Stories from the Greater Manchester Integrated System
Sam Keighley, Strategic Director, Yorkshire Sport Foundation and part of the Sport England Extended Workforce team hosted a panel conversation with Q&A from the audience online and in the room.
The group of local leaders from across health and physical activity sectors in Greater Manchester shared the stories, which Dr. Kath Edgar captured in note form and Hayley has translated below (thanks to Kath!)
 Jan Sinclair
Jan Sinclair
Jan Sinclair is a NHS Senior health care and public health nurse Stepping Hill Hospital in Stockport, and is also Lead Nurse for the PACC programme for OHID. She helps people to live healthier lifestyles at Stepping Hill Hospital and in the Stockport community. She also has a role promoting good health across the country as part of the Moving Medicine work, supporting Physical Activity Champions Training. Via Zoom, Jan reflected on what she has learnt so far about how to change mindsets, beliefs, policy and practice within the health and care workforce? And she shared her learnings about how tools and resources like Moving Medicine and Physical Activity Champion Training can do to support this work? Anything in the way?
What is important and makes change happen?
- Passionate people
- Connections and relationships (eg with Stockport Council)
- Motivation to keep going.
- Strategic context- eg Stockport Active Communities Strategy.
- Keep nudging away!
- Evaluation is key- to understand and evidence that what you are doing is working
- Importance of physical activity has grown (in health sector) because of Covid-19- need to grab this [opportunity] and get momentum going.
- Sharing and raising awareness is key.
- Evidence- there is so much evidence on physical activity is of benefit to patients.
- NICE guidance is really good for clinicians.
- Help clinicians to see this as part of their role- Moving Medicine resources are really useful- useful to have them printed out and visible.
Challenges
- This isn’t flavour of the month with everyone in clinical areas.
- Lots of people are very positive- but we’re battling staff time and commissioning priorities.
Kirsty Rowlinson-Groves and Zoe Merchant then shared their learnings from the development of the GM Prehab4Cancer programme.
Kirsty is the GM Active Programme Manager on Prehab4 Cancer. She is a community-based specialist exercise instructor working with patients with long-term health conditions to improve their physical health and mental wellbeing through exercise and activity.
Zoe is the Programme Lead on Prehab4Cancer for the GM Cancer team.
Together they explained what they have learnt about what matters when bringing together different sectors like this to work to a common purpose. They reflected on the leadership learnings that are be transferable for anyone working to integrate physical activity and health.
What is important and makes change happen?
- Evidence: scientific evidence that if you psychologically, nutritionally and physically prepare, there are much better outcomes.
- Getting clinicians on board.
- Working effectively across sectors- clinicians and community, researchers and practitioners.
- Data sharing and effective systems.
- Test and learn approach resourced by Transformation Funding that enabled the longer term approach.
- The messenger matters: for cancer patients, their oncology team are their ‘gods’, so they need to be on board.
- Patient voice: ppatients told us they didn’t want hospital based and clinical. They wanted to access support in the community.
- Collaboration: GM Active working across the whole area – over 80 leisure sites. Working at scale.
- Evidence and evaluation that this works: thorough [external] evaluation of physical health, clinical outcomes and mortality, with a comparison group. This demonstrated huge benefits: reduced time in hospital, reduced admissions, more likely to be alive at one year etc and could prove it.
- Clinicians are so busy and worn down, but GM Active could say ‘yes’. So refreshing.
- Data is not just numbers. It’s the human voice, patient experience: case studies and experience matter. We needed a narrative along with the data.
- Seek to understand first: asked ‘what will you need to see in an evaluation report’ before designed the process.
Challenges
- Postcode lottery of services previously.
- 10 commissioning conversations rather than 1.
 Sheni Ravji-Smith
Sheni Ravji-Smith
Workforce Wellbeing
Sheni Ravji-Smith is Head of System Organisational Development, Leadership & Wellbeing working across the whole public service system in Greater Manchester, based at NHS GM Integrated Care. She is leading on the Wellbeing and Inclusion system developments across Greater Manchester.
Sheni has been working closely with GreaterSport integrating and embedding active workplace culture change as part of a wider approach to wellbeing. Sheni explained why these matter to the work she leads, how integral physical activity is and how it connects to the key priorities in the ICS approach.
What is important and makes change happen?
- Focus on good wellbeing and work.
- Whole person at home as well as at work.
- Try to shift culture and understand wellbeing is very personal – more inclusive approach – not a homogeneous offer – no what we think people want.
- Think who we can influence and preventative wellbeing – what we can do to support that in the workplace – where we can find that support. Practical activities happening across GM.
- Support people to be more reflective on wellbeing- so physical wellbeing might not be about elite running but simple actions day to day.
- Shift the narrative to prevention – not waiting for it to go wrong.
- Shifting the nature of conversation: from “what is matter with you” to “what matters TO you”
- Data is listening to the people and where we shift attention to.
- Recognise that nature of what ‘work’ looks like now has changed.
- In GM have 180,000 health and care workforce – varying cultures and structures. Huge and micro businesses. We’ve been collating what we have seen and actioned into:
- looking after individuals
- support line mangers to support wellbeing practice
- huge amount of resources but didn’t know how to get it and understand if it was good or relevant so we collated best practice in one place – curating – QA and bringing it together.
- The key is that it shouldn’t matter who and where you work but you can access that support.
Sam asked a final question about scale – what has Sheni learnt?
Sheni said
“we have a huge footprint and need to consider scale. People don’t have resources and capacity to respond to everything so where can we priorities and help people step in the space and take that back with PRACTICAL tools make sure its driven by what the people want and not productivity or absentee – people want to feel valued and heard and priorities and principles”.
“We don’t want a reactive response when things go wrong – we need a culture shift – this is hard and slow work – cumulative steps to shift culture”

Strategy and Vision for Health Creation
Finally, Warren Heppolette, Chief Officer, Strategy and Innovation at NHS Greater Manchester, Trustee at GreaterSport and co-owner of FC United, shared his reflections on the strengths in approach that he has seen and some top tips for anyone starting their journey to develop shared purpose and integration with their ICS.
“What is my role in creating the conditions? For it to be more than sparks that occur when people meet but become routine and expectation across the system”.
Warren explained that there are 42 ICSs now established, and all have to create a strategy. Some strategies will be really clear about physical activity, and some won’t; based on history, relationships and the leadership atmosphere to create conditions that physical activity is in the strategy.
[In GM] we were helped that before ICS’s, we were a devolved city region with health and care already part of this. We established a relationship between Sport England and GreaterSport and GM Moving: we were given grand challenge with what to do health devolution with none of the [current] challenges of national [direction]. So, the strategy in 2015 – asked one question –
“What contributes to good health, who are the people and how we connect them?”.
It was an amazing gift to do this. We were given headspace, freedom to act and attract people. People came to us. They talked about the availability of work, connection of communities, movement and physical activity. Then we needed to find a way to make it work. To plan the conditions that create health rather than [just] create health services.
Warren reflected that we have been encouraged in this way of working: Connection as a habit; introduce parts of the system to each other, develop shared objectives. He referenced Zoe and Kirsty’s Prehab and Rehab examples and how they bring leverage to each other. We need the health service to bring its capacity to an objective on movement and physical activity. With the capacity of leisure providers and trusts etc [we see a] pooling of reciprocal energy and contributions.
Where next?
Now [as Hayley said] we need to stock take what we have done and where we need to go next. There are challenges. Warren acknowledged it can still be a slog and there are some more hearts and minds to change.
We need to
- Lead on evaluation – take people on the intellectual journey – the evidence is there, how do we think beyond?
- Have conversations about what matters to you – e.g. GPs having a million conversations.
- We need to apply what we have learnt and what will the next strategy to achieve scale
- We will have primary care networks now
- People need headspace to engage.
- We need the exemplars and to bring others through a process of change.
Sam asked about the role of GreaterSport, the Active Partnership which Warren is now a Trustee of. He said he has been an enthusiastic advocate for the character of GreaterSport. It’s not just “my job is this”, it’s a progressive organization. GreaterSport came to the GM Health and Social Care Partnership on back of the devolution with a fearlessness; a conversation of how do we make this happen? Then we made progress through unlocking conversations.
An important point made to conclude, is that the community power shift is in its early stages. We need to think seriously beyond services FOR people to a more democratic service powered by community – this is a fairly radical shift and we need to unlock participation.
Finally, Sam asked how important it is to have ‘spark’ conversations.
Warren reflected that it is essential to be inspired. So now Prehab [for Cancer] is [becoming] routine, then we need something else that’s new.
Warren finished with this:
“Tony Wilson said- when you live and work in Manchester, you need to make the inconceivable into the routine”. This is inspiring”
And that felt like a great place to pause and talk to each other. Inspired.
The group went into breakout rooms and round table discussions to consider what they’d heard, what they’d like to hear more about and came back for a Q&A session.
At the end of the morning, the group set their intentions to act and the morning was wrapped up with a sense of gratitude for the brilliant stories that had been shared, and the inspiration we finished with.
At the end of the event, we did a short activity to reflect on what we’d heard and where next. Here is a short summary below:
What have we heard/learnt this morning?
Mindset, Approach and Language
- Long term journey, not short fix
- Need to understand how the system works
- Shift in language required: listening, not telling: what do you need?
- Keep the faith! We’re making progress
- Don’t give up if at first you don’t succeed- keep going when things seem impossible!
- There is already a strong case to be made- make sure enough people hear it and build momentum- have conversations that respond to the different needs of stakeholders
- Changing hearts and minds is key – it’s reassuring (and it isn’t!) that there is still a challenge even when there is clear evidence and pilots have been implemented.
Ways of Working
- Sparks and conversations are key
- Keep nudging away
- [The importance of] listening and storytelling
- The need for a clearer approach on working together: national, regional and local
- Bang the drum for prevention
- Consolidate ideas- for example in working with employers
- Sharing evidence of good practice is key
- Evaluation – both quantitative and qualitative are key
- Evolve the narrative
- Continued conversations and learning with everyone internally and across the system
- Understand individuals and their role and contribution to the agenda- no matter how small- equally important for collective impact
- Place based approaches are important
- Take time to listen and not impose
- Evidence base is essential to convince a clinician
- Ask what they need, don’t assume/tell. Listen first.
- Stakeholder engagement is key
- Work at different levels and see where the conversation goes
And remember…
- Share learning to put into practice
- The useful resources we can use- and work to ensure we support the awareness of those
- [Support people as they] wrestle with what their role in the system should be
Finally, participants shared some of their personal next steps
- Reading the pre-reading (blogs)
- Feedback to Senior Leadership Team and wider teams/stakeholders
- Meet colleagues who were here and reflect on next steps
- Think about the way literature and communication is used
- Think really practically about everything we do- make it as easy as possible for busy people to engage
- Keep engaging in events like this- with those who are already doing the work
- Put together a briefing paper on how we should work across key health bodies
- Continue to work collaboratively in place
- Raise awareness of tools and resources (eg Moving Medicine)
- Learn more about the ICS and who to contact/work within my area
- Help people to figure out how they can contribute to this agenda
- Make the unconventional routine
- Support communities with lived experience to contribute to this agenda
- Learn more about how this evolves
- Speak with clinical partners who are already engaged- understand why they are on board, what has attracted them and how we can engage others.
- Think differently about our (Versus Arthritis) services, how we work with local partners and how we can engage others
- Follow up with the GM examples- use them in our influencing and advocacy work and help to share the learning
- Be curious about our system partners and their motivations/outcomes
- Continue the conversations- see how we can secure positive outcomes for disabled people
- Be a voice for VCSE sector to link them to health
- Start the conversation with [our local colleagues] to see if there is an appetite (ref cancer pathway)
And a few longer-term ambitions
- Hear more about what others are doing
- Measurable, tangible outcomes- eg one PACC training delivered, one PCN intervention with physical activity embedded
- Understand the new systems and what they need to be able to embed physical activity
- Champions across health care like Jan
- Develop long lasting appropriate processes and initiatives that are valued by the community
- Work as a facilitator across workplaces to further embed movement as the norm- addressing and understanding barriers using colleagues GM wide
- Continuation funding – evaluation and data will be important
- Stay true to my core commitment to working in the health and physical activity space
- Contribute to connecting the different parts of the system and learning
- Understand how to influence ICS at various levels without simply ‘selling’ a product
- Sharing good practice as we have done today
- Work more closely with Active Partnerships and the physical activity sector to help to advocate for physical activity in ICS plans
- Ensure people’s voices are heard
- Connect with NHS colleagues to ensure that disabled people’s voices are heard – how they want it, where and with who.
- For every workplace to prioritise wellbeing of their employees and encourage ways to move during working hours
- To ensure that the AP is a member of the [relevant] boards to advocate for place based physical activity connections
Someone said…
“My favourite quote was from Warren: My job isn’t to plan health services. My job is to plan [create] the conditions to create health”
That feels like a great place to finish. Our job is to create the conditions for health creation… I hope this article will help you in your role within that.
Further Information
Twitter thread of learning from GM journey so far (shared on ICS launch day)
Hayley Lever’s live Twitter thread of the opening session
Blog: Integrating physical activity and health and care: our journey so far

